.jpg)
Comprehensive Orthodontic Correction of Class I and Class II Division 1 Malocclusions Using Fixed Mechanotherapy: Case Series
Sharbari Dutta1*  and Brahmananda Dutta2
and Brahmananda Dutta2
1Department of Health Research, International Institute of Health Management Research, New Delhi India .
2Department of Pedodontics and Preventive Dentistry, Kalinga Institute of Dental Sciences, KIIT University, Bhubaneswar, Orissa India .
http://dx.doi.org/0.12944/EDJ.07.0102.10
Malocclusion is one of the most widely prevalent orthodontic problems encountered in adolescents, often affecting dental alignment, function, and facial esthetics. Orthodontics is a vital branch of dentistry, playing an important role in facial esthetics and functional occlusion thus enhancing the overall quality of life. Although Angle’s Class I and Class II Division 1 Occlusal disharmony vary in their clinical presentation, both conditions can be predictably corrected using well-planned extraction strategies and comprehensive fixed appliance therapy.
This paper presents a series of three adolescent orthodontic cases managed with individualized treatment protocols. The first two cases involved are Angle’s Class I malocclusion with mild upper anterior proclination and anterior crowding in both arches, and the other case with mild upper proclination and lower anterior crowding. The third case demonstrated an Angle’s Class II Division 1 occlusal disharmony with upper anterior proclination, increased overjet, and mild lower irregularity. All cases were treated using pre-adjusted edgewise appliances (MBT prescription) with appropriate extractions to create space for alignment and retraction. A planned sequence of archwires along with appropriate elastic forces facilitated controlled and efficient tooth movement during treatment. Post-treatment evaluations revealed well-aligned arches, ideal overjet and overbite, balanced facial profiles, and stable occlusal relationships.
The presented cases highlight the efficacy of fixed mechanotherapy combined with planned extraction in achieving functional and esthetic harmony in adolescent patients with Class I and Class II Division 1 malocclusions. Careful diagnosis, biomechanically controlled tooth movement, and adherence to retention protocols are essential for achieving long-term stability and optimal results.
Copy the following to cite this article:
Dutta S, Dutta B. Comprehensive Orthodontic Correction of Class I and Class II Division 1 Malocclusions Using Fixed Mechanotherapy: Case Series. Dental Journal 2025; 7(1-2).
DOI:http://dx.doi.org/0.12944/EDJ.07.0102.10Copy the following to cite this URL:
Dutta S, Dutta B. Comprehensive Orthodontic Correction of Class I and Class II Division 1 Malocclusions Using Fixed Mechanotherapy: Case Series. Dental Journal 2025; 7(1-2). Available here: https://bit.ly/4qLBdzH
Download article (pdf) Citation Manager

Introduction
In the late nineteenth century, Edward Angle introduced a systematic classification of occlusal disharmony, with four categories: normal/ideal occlusion, Class I, Class II, and Class III, defining ideal occlusion based on the positional relationship between the mesiobuccal cusp of the maxillary first molar and the buccal groove present on the lower first molar.1 Malocclusion is deviation from the ideal occlusion and is a common orthodontic problem encountered in clinical practice. Among these, Angle’s Class I and Class II Division 1 malocclusions constitute most cases seen during adolescence, which is a critical period for interceptive and corrective orthodontic intervention. Class I occlusal disharmony is characterized by a normal molar relationship, but tooth alignment issues such as crowding, spacing, or proclination can still compromise esthetics and occlusal efficiency. Class II Division 1 occlusal disharmony, on the other hand, typically presents with a distal positioning of the lower molars accompanied by forward-inclined maxillary incisors.2
Adolescent patients presenting with such dental malocclusions typically exhibit good skeletal balance with localized dental irregularities or mild skeletal discrepancies that respond well to fixed mechanotherapy. Extraction therapy, when indicated, remains an effective means of gaining space for alignment, relieving crowding, and improving soft-tissue balance. The use of pre-adjusted edgewise appliances (MBT prescription) allow controlled tooth movement with efficient torque, tip, and in-out compensation, leading to stable and esthetically pleasing results.3
The present compilation of three cases (Table 1) demonstrates the orthodontic management of common adolescent malocclusion using systematic biomechanical approaches. The first two cases represent Angle’s Class I malocclusions—one with mild upper proclination and generalized anterior crowding, and another with mild upper proclination and lower anterior crowding. The third case highlights the treatment of an Angle’s Class II Division 1 malocclusion with increased overjet and upper anterior proclination. Through individualized treatment planning involving extractions, sequential arch wire progression, and appropriate retention protocols, all three patients achieved functional occlusion, improved smile esthetics, and long-term stability. As the cases involved adolescent patients, written informed consent was obtained from the parents/guardians along with patient assent. Institutional ethical approval was obtained as per institutional guidelines. All patient data have been anonymized for publication.
Case Report 1
A 12-year-old female patient with irregularly placed upper and lower anterior teeth reported to the Department. Clinical and radiographic examination revealed an Angle’s Class I molar relationship with mild upper anterior proclination and anterior crowding. Cephalometric analysis was done(Table 2). The patient exhibited a Class I skeletal pattern with an average growth pattern, balanced soft-tissue profile, and harmonious facial proportions, confirming a diagnosis of Angle’s Class I occlusal disharmony with mild upper proclination and anterior crowding. The treatment objectives were to relieve anterior crowding, correct upper proclination, achieve ideal alignment and leveling while maintaining Class I molar relation, improve facial aesthetics, and ensure long-term stability. The treatment plan included extraction of all first premolars (namely, 14, 24, 34, and 44) to create space for alignment and retraction, followed by fixed mechanotherapy using pre-adjusted edgewise brackets (MBT prescription). Initial leveling and alignment were carried out with 0.014-inch round NiTi arch wires, followed by progressive 0.016-inch × 0.022-inch arch wire changes. Space closure was accomplished using elastic chains in both arches, with finishing and retention using retainers. The total active treatment duration was approximately 18 months.
Anchorage requirements were moderate. Posterior anchorage was reinforced by consolidating molars and premolars into a single anchorage unit, supported by 0.016-inch × 0.022-inch stainless steel arch wires during space closure. Light, continuous forces from elastic chains prevented unwanted mesial drift, maintaining the Class I molar relationship throughout retraction.
Post-treatment evaluation showed well-aligned arches, ideal overjet and overbite, and maintenance of Class I molar relationship, along with an improved facial profile, balanced lip posture, and enhanced smile aesthetics. Radiographic assessment confirmed good root parallelism and bone support. Retention was provided using a Hawley’s retainer in the upper arch and a fixed lingual bonded retainer in the lower arch, resulting in a stable, functionally efficient, and aesthetically pleasing outcome. (Figure 1-9).
Case Report 1
.jpg) | Figure 1: Pre-operative extraoral views
|
.jpg) | Figure 2: Pre-operative radiograph
|
.jpg) | Figure 3: Pre-operative Orthopantomogram
|
.jpg) | Figure 4a: Occlusal view of maxillary arch
|
.jpg) | Figure 4b: Occlusal view of mandibular arch
|
.jpg) | Figure 4c: Frontal Intraoral view
|
.jpg) | Figure 4d: Right Buccal Intraoral View
|
.jpg) | Figure 4e: Left Buccal Intraoral View
|
.jpg) | Figure 5a: Extraction of 14 and 24 followed by bonding with brackets in upper arch- insertion of 0.014 RCS wire (Occlusal view)
|
.jpg) | Figure 5b: Extraction of 14 and 24 followed by bonding with brackets in upper arch- insertion of 0.014 RCS wire (Frontal view)
|
.jpg) | Figure 5c: Extraction of 34 and 44 followed by bonding with brackets in upper arch- insertion of 0.014 rcs wire
|
.jpg) | Figure 6a: E-chain inserted with respect to upper arch
|
.jpg) | Figure 6b: E-chain inserted with respect to lower arch
|
.jpg) | Figure 6c: E-chain inserted in upper and lower arch (Frontal view)
|
.jpg) | Figure 7a: Closure of extraction spaces on left sides
|
.jpg) | Figure 7b: Closure of extraction spaces on right side
|
.jpg) | Figure 8a: Hawley’s retainer in upper arch (Occlusal view)
|
.jpg) | Figure 8b: Hawley’s retainer in upper arch (Frontal View)
|
.jpg) | Figure 8c: Lingual bonded retainer in the lower arch
|
.jpg) | Figure 9a: Post-Operative Extraoral Views (Frontal View)
|
| Figure 8c: Lingual bonded retainer in the lower arch
|
.jpg) | Figure 9b: Post-Operative Extraoral Views (Lateral View)
|
Case Report 2
A 13-year-old female patient reported to the department with the chief complaint of irregularly placed teeth in the upper and lower arches. Clinical and radiographic examination revealed an Angle’s Class I molar relationship with mild upper anterior proclination and crowding in the lower anterior region. Cephalometric analysis was done(Table 2). The patient demonstrated a Class I skeletal pattern with an average growth tendency and a balanced soft-tissue profile, confirming the diagnosis of Angle’s Class I malocclusion with mild upper proclination and lower anterior crowding. The primary treatment objectives were to relieve lower anterior crowding, correct upper proclination, establish ideal alignment and leveling of both arches, maintain Class I molar relation, and enhance facial and smile aesthetics while ensuring long-term stability.
Table 1: Comparative Summary of Orthodontic Case Reports
Patient ID | Age | Angle’s Classification | Key Dental Findings | Skeletal Pattern | Soft-Tissue Profile | Treatment Summary |
Patient 1 | 14 years | Angle’s Class I malocclusion | Mild upper anterior proclination and crowding in both arches | Class I, average growth | Balanced and harmonious | Extraction of all first premolars (14, 24, 34, 44); fixed mechanotherapy with MBT brackets; space closure using elastic chains; Hawley’s and fixed retainers used |
Patient 2 | 13 years | Angle’s Class I malocclusion | Mild upper anterior proclination and lower anterior crowding | Class I, average growth | Balanced soft-tissue profile | Extraction of all first premolars (14, 24, 34, 44); fixed appliance therapy with MBT brackets; sequential archwire changes and space closure with elastic chains; Hawley’s and fixed retainers |
Patient 2 | 13 years | Angle’s Class II Division 1 malocclusion | Upper anterior proclination, increased overjet, and mild lower irregularity | Class II, average growth | Convex profile with mild lip incompetence | Extraction of upper right lateral incisor (12); fixed mechanotherapy with MBT brackets; NiTi wires and box elastics used; retention with Hawley’s and fixed lingual retainer |
Cephalometric Parameter | Typical Range | Case 1 (Angle’s Class 1) | Case 2 (Angle’s Class 1) | Case 3(Angle’s Class II Div 1) |
SNA (°) | 80–82° | 82° | 82.0 ° | 79.6° |
SNB (°) | 78–80° | 80° | 80.9 ° | 71.0° |
ANB (°) | 2–4° | 2° (Skeletal Class I) | 1.6° (Skeletal Class I) | 8.6° (Skeletal Class II) |
IMPA (°) | 90–100° | 101° (mild proclination) | 99.0 ° (mild proclination) | 96.1° |
The treatment plan included extraction of all first premolars (14, 24, 34, and 44) to create space for retraction and alignment. Fixed mechanotherapy was carried out using pre-adjusted edgewise brackets (MBT prescription). After the extraction of 14 and 24, the upper arch was bonded and 0.014-inch round NiTi wires were placed for initial leveling. Subsequently, 34 and 44 were extracted, and brackets were bonded in the lower arch with insertion of 0.014-inch round NiTi wires. Progressive arch wire changes were made to 0.016-inch round arch wire followed by rectangular 0.016-inch × 0.022-inch arch wires in the upper arch for torque and finishing control. Elastic chains were placed from canine to first molar in both arches to achieve space closure.
Moderate anchorage was necessary for upper incisor retraction. The posterior teeth were consolidated into a unified anchorage block, and rectangular stainless steel wires were used during retraction to resist anchorage loss. Elastomeric chains were applied in controlled intervals, allowing efficient space closure while maintaining posterior anchorage.
Regular follow-ups were conducted for wire progression and monitoring of tooth movement. The total active treatment period lasted approximately 18 months.
Post-treatment evaluation revealed well-aligned arches, ideal overjet and overbite, and maintenance of the Class I molar relationship. Facial profile improved significantly with balanced lip posture and pleasing smile aesthetics. Post-treatment radiographs showed good root parallelism and bone support. Retention was provided using a Hawley’s retainer in the upper arch and a lingual bonded retainer in the lower arch to maintain alignment and minimize the risk of relapse. The treatment successfully met all objectives, resulting in improved dental alignment, enhanced facial harmony, and a stable, functional, and aesthetic occlusion. (Figure 10-18).
Case Report 2
 | Figure 10a: Pre-Operative Extraoral (Frontal) Views
|
 | Figure 10b: Pre-Operative Extraoral(Lateral) Views
|
 | Figure 11a: Pre-operative occlusal view of maxillary arch
|
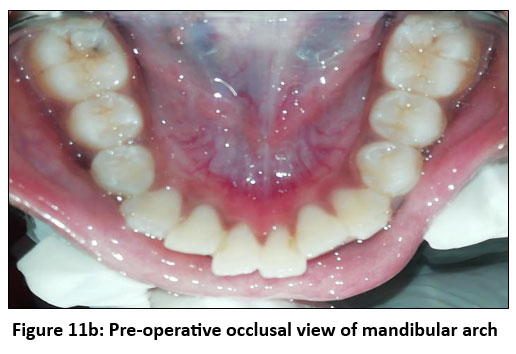 | Figure 11b: Pre-operative occlusal view of mandibular arch
|
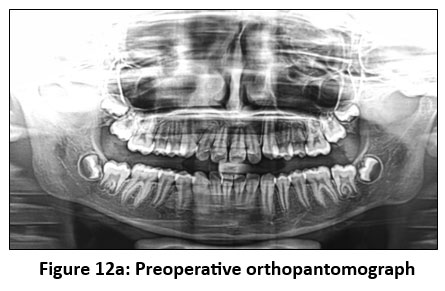 | Figure 12a: Preoperative orthopantomograph
|
 | Figure 12b: Preoperative lateral cephalogram
|
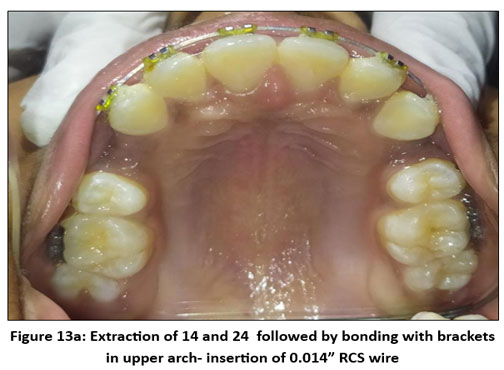 | Figure 13a: Extraction of 14 and 24 followed by bonding with brackets in upper arch- insertion of 0.014” RCS wire
|
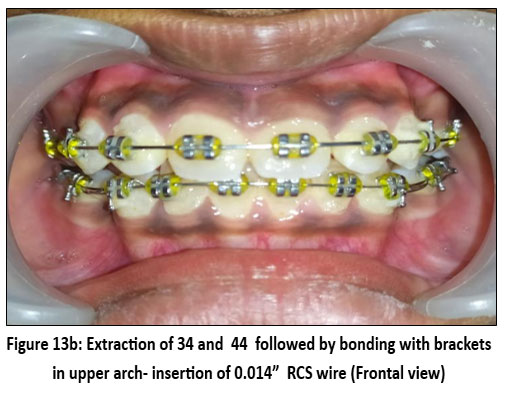 | Figure 13b: Extraction of 34 and 44 followed by bonding with brackets in upper arch- insertion of 0.014” RCS wire (Frontal view)
|
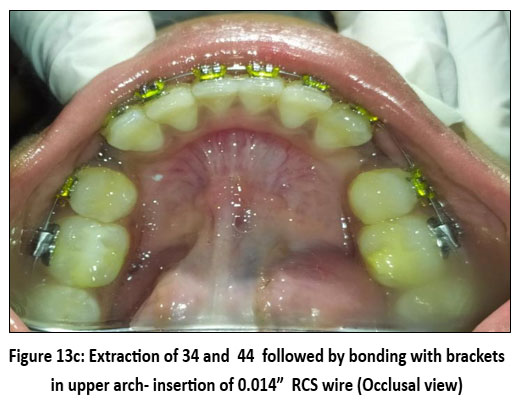 | Figure 13c: Extraction of 34 and 44 followed by bonding with brackets in upper arch- insertion of 0.014” RCS wire (Occlusal view)
|
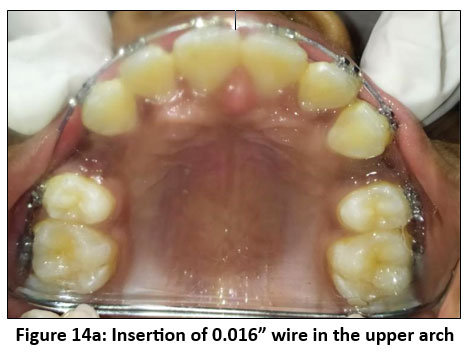 | Figure 14a: Insertion of 0.016” wire in the upper arch
|
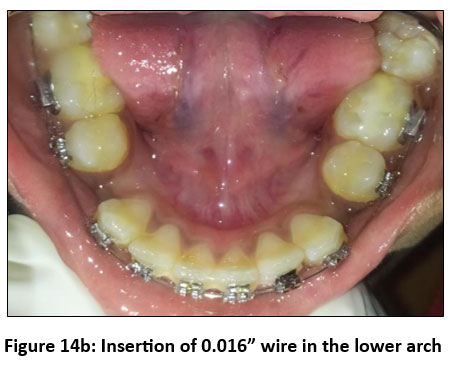 | Figure 14b: Insertion of 0.016” wire in the lower arch
|
 | Figure 15: E-chain inserted from canine to first molar
|
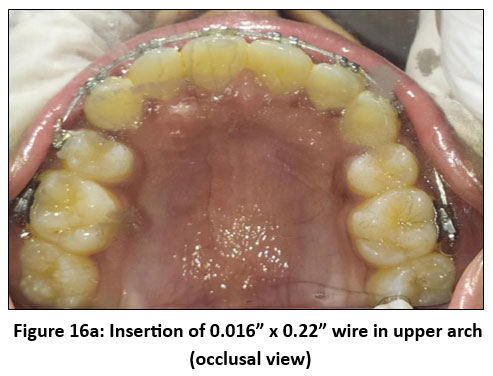 | Figure 16a: Insertion of 0.016” x 0.22” wire in upper arch (occlusal view)
|
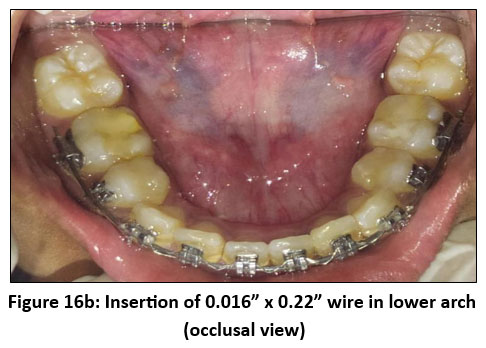 | Figure 16b: Insertion of 0.016” x 0.22” wire in lower arch (occlusal view)
|
 | Figure 16c: Insertion of 0.016” x 0.22” wire in upper and lower arch (frontal view)
|
 | Figure 17a: Hawley’s retainer in upper arch (Occlusal view)
|
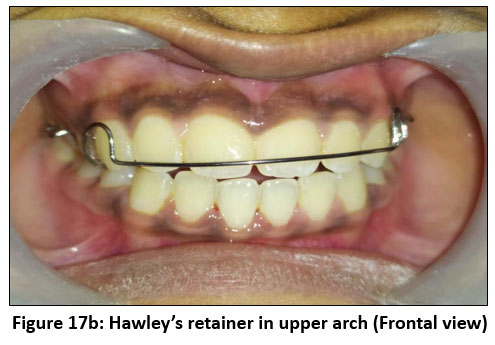 | Figure 17b: Hawley’s retainer in upper arch (Frontal view)
|
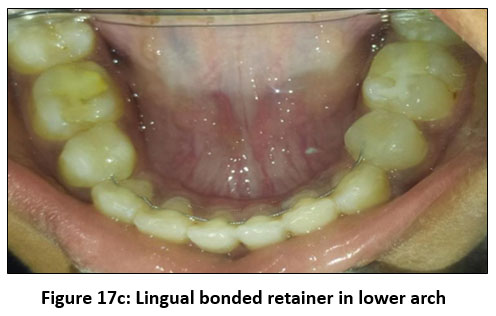 | Figure 17c: Lingual bonded retainer in lower arch
|
 | Figure 18a: Post-operative extraoral views (Frontal view)
|
 | Figure 18b: Post-operative extraoral views (Lateral View)
|
Case Report 3
A 13-year-old female patient reported to the department with the chief complaint of forwardly placed upper front teeth and irregular lower anterior alignment. Clinical and radiographic examination revealed an Angle’s Class II Division 1 occlusal disharmony characterized by proclined upper anterior teeth, increased overjet, and mild lower anterior irregularity. Cephalometric analysis was done (Table 2). The patient exhibited a Class II skeletal pattern with an average growth tendency, convex facial profile, and potentially strained lip competence, confirming the diagnosis of Angle’s Class II Division 1 occlusal disharmony.
The treatment objectives were to reduce upper anterior proclination and overjet, achieve alignment and leveling in both arches, establish Class I canine and molar relationships, improve lip competence, and enhance facial esthetics while maintaining long-term stability. The treatment plan involved extraction of the upper right lateral incisor (to correct asymmetry and crowding) followed by bonding of pre-adjusted edgewise brackets in the upper arch. A co-axial arch wire was initially placed for mild alignment. The lower arch was then bonded and aligned using 0.014-inch round NiTi wire, while a 0.016-inch × 0.022-inch NiTi wire was used in the upper arch for controlled retraction and torque correction. Interarch mechanics in the form of box elastics were used to coordinate the arches and correct occlusal discrepancies. Progressive arch wire changes were made to 0.016-inch round arch wire followed by rectangular 0.016-inch × 0.022-inch arch wires in the upper arch for torque and finishing control.
Extraction of the upper right lateral incisor (12) was selected due to the patient's unilateral anterior crowding, significant maxillary incisor proclination, and dental asymmetry. Removing 12 provided direct space for controlled retraction of the central incisor and canine on the right side, allowing correction of the midline and improvement of anterior alignment without the need for complex asymmetric mechanics. Biomechanically, lateral incisor extraction simplifies anterior retraction by reducing force imbalances and enabling more predictable correction of proclination. Literature supports lateral incisor extraction in cases with tooth-size discrepancy, compromised lateral incisor position, or asymmetric crowding, as it enhances esthetic and functional outcomes while preserving canine guidance.
Significant anchorage was required due to the need for marked retraction following unilateral extraction of 12. Posterior anchorage was reinforced by consolidating molars and premolars, supported by progression to rectangular stainless steel archwires. Interarch box elastics supplemented occlusal coordination without significantly compromising anchorage. This approach ensured controlled anterior retraction and preservation of the existing molar relation.
The active treatment spanned approximately five months, after which satisfactory alignment, correction of anterior proclination, and normalization of overjet and overbite were achieved. Post-treatment records showed a balanced facial profile, improved smile esthetics, and proper intercuspation with a functional and stable occlusion. Radiographs revealed good root alignment and parallelism. Retention was maintained using a Hawley’s retainer in the upper arch and a fixed lingual bonded retainer in the lower arch to prevent relapse.
The overall treatment outcome demonstrated successful correction of the Class II Division 1 occlusal irregularity, resulting in enhanced facial harmony, improved dental function, and stable long-term aesthetics within a short duration of therapy. (Figure 19-26).
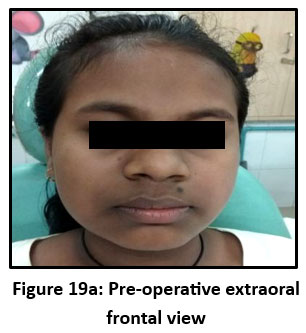 | Figure 19a: Pre-operative extraoral frontal view
|
 | Figure 19b: Pre-operative extraoral lateral view
|
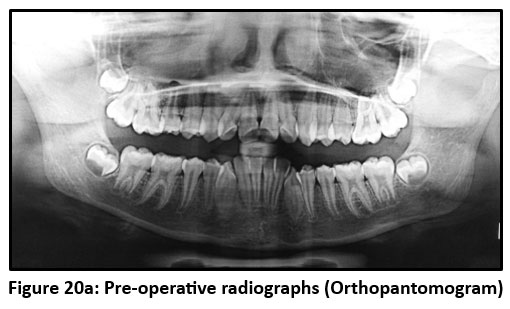 | Figure 20a: Pre-operative radiographs (Orthopantomogram)
|
 | Figure 20b: Pre-operative radiographs (Lateral Cephalogram)
|
 | Figure 21a: Pre-operative intraoral views (Frontal View)
|
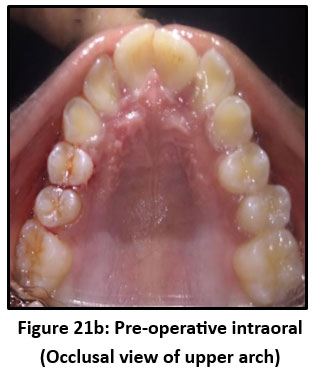 | Figure 21b: Pre-operative intraoral (Occlusal view of upper arch)
|
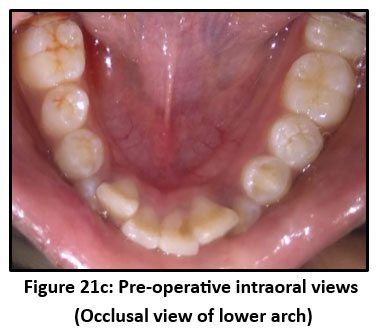 | Figure 21c: Pre-operative intraoral views (Occlusal view of lower arch)
|
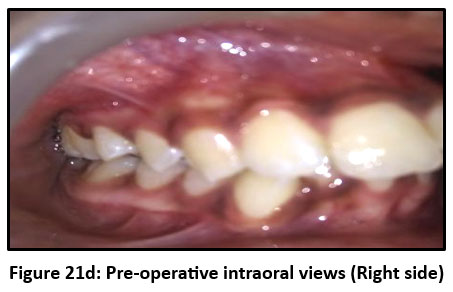 | Figure 21d: Pre-operative intraoral views (Right side)
|
 | Figure 21e: Pre-operative intraoral views (Left side)
|
 | Figure 22a: Extraction of 12
|
 | Figure 22b: Bonding with brackets in upper arch- insertion of co-axial wire
|
 | Figure 23a: Bonding with brackets of lower arch and insertion of 0.012” wire and 16-22 NiTi in upper arch /9Frontal view).
|
 | Figure 23b: Box elastics given (Right side)
|
| Figure 23b: Box elastics given (Right side)
|
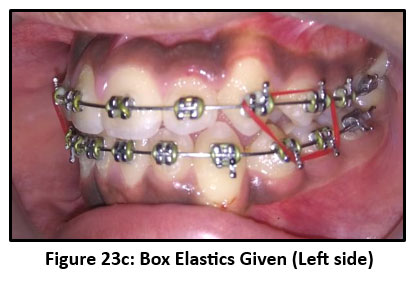 | Figure 23c: Box Elastics Given (Left side)
|
 | Figure 24a: Frontal view following debonding after 5 months
|
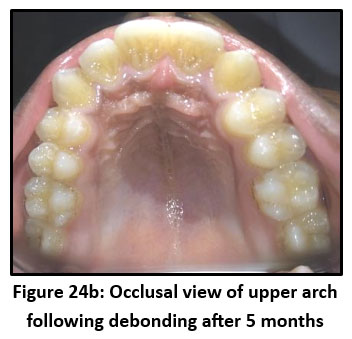 | Figure 24b: Occlusal view of upper arch following debonding after 5 months
|
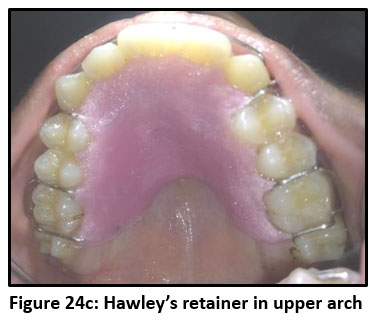 | Figure 24c: Hawley’s retainer in upper arch
|
 | Figure 24d: lingual bonded retainer in lower arch
|
 | Figure 25a: Post-operative intraoral views
|
 | Figure 25b: Post-operative intraoral views
|
Discussion
The three cases presented illustrate the versatility of fixed mechanotherapy in managing both Class I and Class II Division 1 occlusal irregularity in adolescents. Each case was approached with individualized treatment objectives while maintaining fundamental orthodontic principles of space management, controlled tooth movement, and retention stability.
In Class I malocclusions (Cases 1 and 2), the molar relationship was already favorable; hence, treatment was primarily aimed at relieving anterior crowding and correcting upper proclination to improve alignment and smile esthetics. Extraction of first premolars (14, 24, 34, 44) was planned to create sufficient space for retraction and leveling. The use of pre-adjusted edgewise MBT brackets with NiTi archwires ensured efficient alignment with light continuous forces, minimizing root resorption and patient discomfort. Sequential archwire progression and the use of elastic chains for space closure allowed optimal control of tooth movement. Post-treatment evaluation confirmed ideal overjet, overbite, and improved facial harmony, demonstrating the efficacy of extraction-based therapy in resolving crowding and achieving stable occlusal relationships. In cases where all first premolars are extracted, the therapeutic aim is usually to finish with a Class I molar relationship, irrespective of the patient’s initial anteroposterior dental alignment. However, since correcting the AP discrepancy can be challenging, this extraction approach should be used carefully in patients whose starting molar relationship is far from Class I and who have limited or no remaining growth. In such situations, extracting premolars in only one arch may provide a more favorable occlusal outcome.4
Class II malocclusion are frequently encountered in clinical orthodontic practice, with epidemiological data suggesting a prevalence of roughly 13–24%.5 The Class II Division 1 case (Case 3) required a different biomechanical approach. The key concern was excessive overjet caused by proclined maxillary incisors and a mild skeletal discrepancy. Reduction of excessive overjet is a primary treatment objective in Class II Division 1 malocclusion, as increased overjet is associated with compromised facial esthetics, lip incompetence, and a higher risk of incisal trauma.6 In the present case series, Case 3 demonstrated a marked reduction in overjet following controlled retraction of the maxillary anterior segment after strategic extraction. The correction was achieved predominantly through dentoalveolar changes rather than skeletal modification, which is consistent with adolescent patients exhibiting mild to moderate skeletal discrepancies and average growth patterns.
Published literature reports that extraction-based fixed mechanotherapy can produce overjet reductions ranging from 4 to 7 mm in adolescent Class II Division 1 patients, depending on initial severity and anchorage control. The outcome observed in this case aligns well with these findings, as space creation through extraction enabled efficient incisor retraction, improvement in lip posture, and establishment of functional overjet without compromising posterior occlusion.7
Space management and incisor retraction were prioritized to correct the sagittal discrepancy and improve lip competence. Extraction of a single upper lateral incisor (12) was performed to correct asymmetry and allow controlled anterior retraction.8 Interarch box elastics played a crucial role in achieving proper intercuspation and coordination between the arches. Despite a shorter active treatment duration, the desired occlusal and esthetic outcomes were achieved efficiently.
Space closure in extraction cases is influenced significantly by archwire material and force delivery systems. In the present cases, initial alignment and early space closure were carried out using nickel–titanium (NiTi) archwires due to their super elasticity and ability to deliver light, continuous forces over a longer activation range. NiTi wires are well documented to enhance patient comfort, reduce chairside adjustments, and promote biologically favorable tooth movement during the initial and intermediate phases of treatment.
As treatment progressed, stainless steel rectangular archwires were introduced to provide greater rigidity, improved torque control, and enhanced anchorage during space closure and finishing stages. Literature indicates that while NiTi wires are more efficient for early alignment, stainless steel wires offer superior control during en-masse retraction and space consolidation. The sequential use of NiTi followed by stainless steel wires in this case series reflects an evidence-based approach that balances efficiency with biomechanical precision, resulting in controlled space closure and optimal root parallelism.9
Long-term stability following orthodontic extraction therapy in adolescents depends on multiple factors, including growth status, quality of finishing, occlusal intercuspation, and adherence to retention protocols. Studies have shown that extraction cases, when properly planned and executed, do not exhibit higher relapse rates than non-extraction treatments and may demonstrate improved stability in cases of severe crowding or proclination.10
In the present case series, stability was addressed through careful finishing, achievement of ideal overjet and overbite, maintenance of proper interdigitation, and the use of appropriate retention appliances. The combination of removable Hawley retainers in the upper arch and fixed lingual bonded retainers in the lower arch is supported by literature as an effective strategy to minimize relapse, particularly in the mandibular anterior region, which is most prone to post-treatment irregularity.
The favorable post-treatment occlusal relationships and retention protocols employed suggest a low risk of relapse, reinforcing the view that adolescent extraction therapy, when biomechanically sound and retention-conscious, can yield stable and long-lasting outcomes.
Across all three cases, the importance of retention was emphasized. A combination of Hawley’s retainer in the upper arch and fixed lingual bonded retainer in the lower arch was used to maintain results and minimize relapse potential. The improvements in soft-tissue profile and smile esthetics reflected successful orthodontic management not only from a dental perspective but also in enhancing facial balance.11
These cases collectively underscore that careful diagnosis, appropriate extraction decisions, and controlled mechanics can produce highly satisfactory results even in seemingly complex occlusal irregularity. The consistent use of light forces, adequate anchorage, and planned wire sequencing remains the cornerstone of achieving efficient and stable orthodontic outcomes.
Conclusion
Successful orthodontic results depend heavily on precise diagnostic evaluation, a tailored treatment plan, and the application of appropriate biomechanical principles. The three adolescent cases presented—two of Class I occlusal irregularity with varying crowding patterns and one of Class II Division 1 occlusal irregularity —demonstrate that both dental and facial harmony can be successfully restored using systematic extraction therapy and fixed mechanotherapy. Proper arch coordination, controlled space closure, and adherence to retention protocols are vital to ensure long-term stability.12 Overall, the treatments produced well-balanced occlusions, better smile profiles, and noticeable improvements in patient self-confidence, reflecting the effectiveness of comprehensive orthodontic management in adolescent occlusal irregularity.
The authors sincerely acknowledge International Institute of Health Management Research (IIHMR), Delhi and the Kalinga Institute of Dental Sciences (KIDS) for their continuous guidance, academic support, and encouragement throughout the development of this paper. Their valuable inputs, clinical supervision, and institutional resources played an essential role in the successful completion of this work.
Funding Source
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
The authors do not have any conflict of interest
Ethics Statement
The paper is based on the clinical treatment provided in our department. It is a case series and not an original study so Ethical clearance was not needed for these cases included in our case series. We cannot provide Ethical clearance for the same.
References
- De Ridder L, Aleksieva A, Willems G, Declerck D, Cadenas De Llano-Pérula M. Prevalence of Orthodontic Malocclusions in Healthy Children and Adolescents: A Systematic Review. IJERPH. 2022;19(12):7446. doi:10.3390/ijerph19127446
- De Ridder L, Aleksieva A, Willems G, Declerck D, Cadenas De Llano-Pérula M. Prevalence of Orthodontic Malocclusions in Healthy Children and Adolescents: A Systematic Review. IJERPH. 2022;19(12):7446. doi:10.3390/ijerph19127446
- Ghodasra R, Brizuela M. Orthodontics, Malocclusion.
- Alnefaie M, Han WJ, Ahn YS, Baik WK, Choi SH. Orthopedic and Nonsurgical Orthodontic Treatment of Adolescent Skeletal Class III Malocclusion Using Bone-Anchored Maxillary Protraction and Temporary Anchorage Devices: A Case Report. Children. 2022;9(5):683. doi:10.3390/children9050683
- Janson G, Nakamura A, Barros SE, Bombonatti R, Chiqueto K. Efficiency of Class I and Class II malocclusion treatment with four premolar extractions. J Appl Oral Sci. 2014;22(6):522-527. doi:10.1590/1678-775720130544
- Badri MK. Effective and Efficient Correction of Severe Skeletal Class II Division 1 Malocclusion with Intermaxillary Elastics. Zawawi K, ed. Case Reports in Dentistry. 2021;2021(1):6663563. doi:10.1155/2021/6663563
- Bittencourt Neto ACD, Saga AY, Pacheco AAR, Tanaka O. Therapeutic approach to Class II, Division 1 malocclusion with maxillary functional orthopedics. Dental Press J Orthod. 2015;20(4):99-125. doi:10.1590/2176-9451.20.4.099-125.sar
- Peter E. One Phase Treatment of Adolescent Class II Malocclusion Using Twin-Block Appliance and Preadjusted Edgewise Appliance—A Case Report. J Indian Orthod Soc. 2022;56(1):71-81. doi:10.1177/03015742221075238
- Konstantonis D, Anthopoulou C, Makou M. Extraction decision and identification of treatment predictors in Class I malocclusions. Prog Orthod. 2013;14(1):47. doi:10.1186/2196-1042-14-47
- Wichelhaus A, Dulla M, Sabbagh H, Baumert U, Stocker T. Stainless steel and NiTi torque archwires and apical root resorption. J Orofac Orthop. 2021;82(1):1-12. doi:10.1007/s00056-020-00244-4
- Bonadio MF, Cotrin P, Marín Ramirez CM, et al. The Influence of Occlusal Adjustment on Long-term Post-treatment Stability of Orthodontic Treatment. TODENTJ. 2023;17(1):e187421062308310. doi:10.2174/18742106-17-231009-2023-44
- Mohanty B, Ravuri P, Kubavat AK, et al. Evaluation of Orthodontic Retention Protocols and Their Impact on Treatment Stability: Insights from a Tertiary Care Study. Journal of Pharmacy and Bioallied Sciences. 2024;16(Suppl 3):S1997-S1999. doi:10.4103/jpbs.jpbs_271_24
- Gandedkar NH, Darendeliler MA. Space gaining in orthodontic treatment planning: The SPEED-L decision-making framework. Seminars in Orthodontics. Published online October 2025:S1073874625001252. doi:10.1053/j.sodo.2025.10.008





