.jpg)
Primary Intraosseous Carcinoma of the Maxilla Derived from an Odontogenic Keratocyst: Clinicopathologic Insights (OKC), Odontogenic Cysts and Tumors, Maxilla
Hyandavi Balla1*  , Divya Uppala1 , Sreekanth Kotina1 and Mahesh Nirujogi2
, Divya Uppala1 , Sreekanth Kotina1 and Mahesh Nirujogi2
1Department of Oral Pathology and Microbiology, GITAM Dental College and Hospital, Visakhapatnam, Andhra Pradesh India .
2Private Practitioner, Visakhapatnam, Andhra Pradesh India .
http://dx.doi.org/10.12944/EDJ.07.0102.08
Primary intraosseous squamous cell carcinoma (PIOSCC) is an uncommon malignant neoplasm arising within the jawbone, without initial connection to the oral mucosa. It is believed to originate from the malignant transformation of odontogenic epithelial remnants, cysts, or tumors. Involvement of the maxilla is exceedingly rare compared to the mandible. The clinical presentation and radiographic features of PIOSCC are often variable and non-specific, which may complicate early diagnosis and lead to confusion with other odontogenic or inflammatory lesions. This case report describes a rare occurrence of PIOSCC developing from an odontogenic keratocyst (OKC) in the maxilla of a 35-year-old female patient. The report discusses the possible mechanisms underlying malignant transformation within odontogenic cysts, emphasizes the biological behavior of this neoplasm, and delineates the characteristic clinical, radiological, and histopathological findings associated with this rare entity.
Copy the following to cite this article:
Balla H, Uppala D, Kotina S. Primary Intraosseous Carcinoma of the Maxilla Derived from an Odontogenic Keratocyst: Clinicopathologic Insights (OKC), Odontogenic Cysts and Tumors, Maxilla. Enviro Dental Journal 2025; 7(1).
DOI:http://dx.doi.org/10.12944/EDJ.07.0102.08Copy the following to cite this URL:
Balla H, Uppala D, Kotina S. Primary Intraosseous Carcinoma of the Maxilla Derived from an Odontogenic Keratocyst: Clinicopathologic Insights (OKC), Odontogenic Cysts and Tumors, Maxilla. Enviro Dental Journal 2025; 7(1). Available here: https://bit.ly/4a0nn7c
Download article (pdf) Citation Manager

Introduction
Primary intraosseous squamous cell carcinoma (PIOSCC) developing from odontogenic cysts or tumors is an uncommon neoplasm of the head and neck, with maxillary involvement being exceptionally rare. The clinical and radiographic characteristics of these lesions often exhibit considerable variation, posing diagnostic challenges. It accounts for less than 2% of all oral squamous cell carcinomas, with maxillary involvement being particularly uncommon compared to the mandible. Because of its low prevalence and varied clinical–radiographic presentation, PIOSCC often mimics benign odontogenic cysts or chronic inflammatory lesions, leading to frequent diagnostic delays or misinterpretation.1
Case-Report
A 35-year-old female patient reported to the outpatient department with a chief complaint of pain and swelling in the right upper anterior tooth region for the past two months and swelling in the same area for four days. Extraoral examination revealed a diffuse swelling involving the middle one-third of the face on the right side. Intraoral examination showed an ill-defined swelling extending anteroposteriorly from the distal aspect of the right central incisor to the mesial aspect of the right second premolar, and superoinferiorly from the buccal vestibule up to the attached gingiva, resulting in vestibular obliteration. An unhealed extraction socket was also noted in the affected region. (Figure 1).
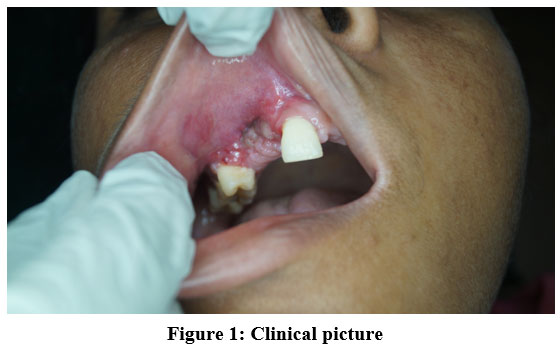 | Figure 1: Clinical picture
|
On palpation, the swelling was found to be tender, firm to hard in consistency, and neither compressible nor reducible. Radiographic investigations were performed and an ill defined radiolucency with ill defined borders was seen, extending from the midline to the mesial side of the 2nd premolar mesiodistally and superioinferiorly extends 0.4 cms away from the floor of the maxillary sinus to the alveolar ridge (Figure 2) and patients previous radiograph is showing a well defined unilocular radiolucency with impacted canine.
 | Figure 2: OPG of the lesion
|
Following routine hematological investigations, an incisional biopsy was performed. The hematoxylin and eosin (H&E)–stained soft tissue section revealed demonstrated parakeratinised corrugated cystic lining epithelium with basal columnar cells arranged in picket fence appearance (Figure 3).
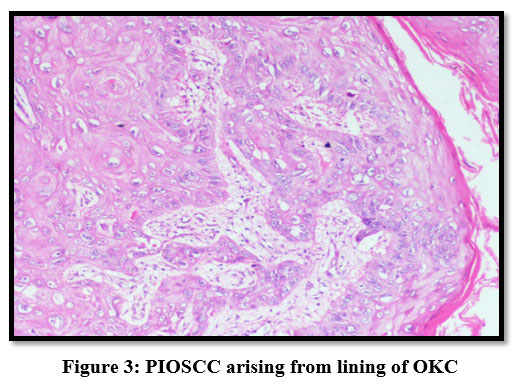 | Figure 3: PIOSCC arising from lining of OKC
|
The connective tissue is infiltrated with neoplastic epithelial cells arranged in the form of islands, cords & sheets. The epithelial islands showed dysplastic features like increased mitotic figures, increased nuclear cytoplasmic ratio, hyper chromatic nucleus, and many keratin pearls.
A final diagnosis of PIOSCC arising from OKC was made and the patient was operated by wide surgical resection of maxilla along with radiotherapy and chemotherapy and she is under follow up.
Discussion
The History of primary intra osseous squamous cell carcinoma (PIOSCC) begins in the year 1913 and described by the Shambhulingappa P, as features consistent with a central (intraosseous) epidermoid carcinoma of the jaw, later renamed as intraalveolar epidermoid carcinoma and PIOSCC by Willis in 1948, Pindborg 1971 respectively.1
And subsequent contribution by the Elzay (1982), Slootweg and Muller (1984) & Waldron and Mustoe(1989) towards the classification of PIOSCC came to end with the replacement of the old terms by the WHO (2005) and is sub- classified as (i) a solid type, (ii) SCC arising from epithelial odontogenic tumours and (iii) SCC derived from odontogenic cysts. Whereas according to recent epithelial odontogenic cysts and tumors given by WHO (2005), OKC had been reclassified as the OKC.2
The diagnosis of primary intraosseous squamous cell carcinoma (PIOSCC) requires careful exclusion of other possible sources of squamous cell carcinoma involving the jaw. The most widely accepted diagnostic criteria were first proposed by Waldron and Mustoe (1989), and later refined by Suei et al. (1994).
To qualify as a PIOSCC the following three criteria should be fulfilled.3,4
There should not be any connections like ulcers with the overlying mucosa, skin or nasal or antral mucosa except causes like trauma and tooth extractions to demarcate it from SCC of surface mucosal origin.
The possibility of metastatic spread from a distant primary site should be excluded through thorough physical examination and advanced imaging modalities such as computed tomography (CT) and magnetic resonance imaging (MRI).
There should be a direct transition from the normal epithelial lining to invasive carcinoma while diagnosing the squamous cell carcinoma has arisen from a OKC.
In the present case, all three criteria were fulfilled. Clinically and radiographically, the lesion was confined to the maxilla, with no mucosal ulceration or evidence of a primary tumor elsewhere in the body. Histopathological examination revealed islands and nests of malignant squamous epithelial cells arising within the cystic lining of an odontogenic keratocyst (OKC), confirming its odontogenic origin. These findings, in conjunction with the absence of distant metastasis, support the diagnosis of PIOSCC arising from an odontogenic keratocyst.
Histologically, the lesion characteristically demonstrates a keratinizing, well-differentiated squamous cell carcinoma associated with an odontogenic keratocyst (OKC). The principal differential diagnoses to be considered include keratoameloblastoma, squamous odontogenic tumor, and central high-grade mucoepidermoid carcinoma. They are excluded by absence of peripheral palisading cells with reverse polarization in the connective tissue tumor islands or sheets, cystic degeneration and foci of calcification, foci of mucous and intermediate cells respectively and metastatic lesions are excluded by negative PET scan reports.3, 5
Pathogenesis of PIOSCC EX OKC is still largely unknown. However, according to Gardner, long standing inflammation may be responsible factor for the malignant transformation.6 In which it includes the formation of reactive oxygen species and metabolites, causing the damage to the DNA genetic material, protein, and cell membranes and eventually it shows compensatory proliferative response of neoplastic cells against the normal programmed cell death (apoptosis) mechanism.2
According to Waldron and Mustoe review of 36 cases of malignant transformation in odontogenic cysts the 2-year survival rate of 53% if lymph node was positive.7 Wide maxillary resection has to be done along with the radiotherapy and chemotherapy. Regular follow up is required in these types of cases.
Conclusion
This report highlights the importance of careful histopathological examination the entire section of innocuous odontogenic cysts because of the possibility carcinomatous changes in their epithelial lining.
Acknowledgement
The authors would like to thank Oral Pathology and Microbiology Department, GITAM Dental College and Hospital for providing academic support and research facilities during the course of this study.
Funding Sources
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of Interest
The authors do not have any conflict of interest.
Data Availability Statement
This statement does not apply to this article.
Ethics Statement
This research did not involve human participants, animal subjects, or any material that requires ethical approval
Informed Consent Statement
Informed consent was obtained from the patient prior to writing of manuscript
Authors’ Contribution
Hyandavi Balla: Conceptualization, Methodology
Divya Uppala: Supervision.
Sreekanth Kotina: Data Collection
Mahesh Nirujogi: Writing – Original Draft.
References
- Shambhulingappa P, Sheikh S, Puri N, Jindal SK. Primary intraosseous carcinoma of the mandible: An update on review of literature with a case report. J Clin Exp Dent. 2010;2(2):e91–e95.
CrossRef - Tamgadge S, Tamgadge A, Modak N, Bhalerao S. Primary intraosseous squamous cell carcinoma arising from an odontogenic keratocyst: A case report and literature review. ecancermedicalscience. 2013;7:316.
- Reichart PA, Philipsen HP. Odontogenic Tumors and Allied Lesions. London, UK: Quintessence Publishing; 2004:233–238.
- Suei Y, Tanimoto K, Taguchi A, Wada T. Primary intraosseous carcinoma: Review of the literature and diagnostic criteria. J Oral Maxillofac Surg. 1994;52:580–583.
CrossRef - Keszler A, Piloni MJ. Malignant transformation in odontogenic keratocysts: Case report. Med Oral. 2002;7(5):331–335.
- Gardner AF. The odontogenic cyst as a potential carcinoma: A clinicopathologic appraisal. J Am Dent Assoc. 1969;78:746–755.
CrossRef - Yu JJ, Hwan EH, Lee SR, Choi JH. Squamous cell carcinoma arising in an odontogenic cyst. Korean J Oral Maxillofac Radiol. 2003;33:235–238.
- Waldron CA, Mustoe TA. Primary intraosseous carcinoma of the mandible with probable origin in an odontogenic cyst. Oral Surg Oral Med Oral Pathol. 1989;67:716–724.
CrossRef





